Better workplace conditions for long-term eldercare staff are key to promoting resident safety amid the coronavirus pandemic

Overview
Residents and workers in long-term residential eldercare settings account for more than 40 percent of all the deaths in the United States due to COVID-19, the disease spread by the new coronavirus—more than 35,000, as of May 21, 2020. This particularly tragic consequence of the coronavirus pandemic sadly illustrates the scale of how the well-being of workers and nursing home residents are deeply intertwined—shedding light on some health and safety concerns that have plagued long-term residential care facilities for more than 60 years.
Policymakers, public health officials, and the American public are still grappling with the ongoing pandemic, which may not abate until there is a proven vaccine provided to large segments of the U.S. population. So, going forward, what can be done to improve the quality of care in long-term residential eldercare settings? My new working paper, “Higher Wages, Service Quality, and Firm Profitability: Evidence from Nursing Homes and Minimum Wage Reforms,” explores one such possibility. In my paper, I show that increasing wages for direct-care staff can improve the safety and health of both nursing home workers and residents. A modest cost increase for providing care would have significant positive impacts.
Download FileBetter workplace conditions for long-term eldercare staff are key to promoting resident safety amid the coronavirus pandemic
In this issue brief, I describe my paper’s key findings, relate these findings to the current healthcare crisis, and conclude with a discussion of potential policy reforms. Briefly, my paper finds that higher minimum wages would increase pay and tenure among eldercare nursing home staff (primarily nursing assistants) without reducing the number of workers or the time nursing staff spends with patients. What’s more, these earnings gains and greater firm-specific expertise benefit consumers by reducing the number of health inspection violations, the prevalence of pressure ulcers and infections, and the number of deaths among nursing home residents.
My preliminary data show that eldercare facilities with more health inspection violations and lower staffing ratios are more likely to experience outbreaks of COVID-19, yet some facilities with known COVID-related deaths are among the highest-ranked providers in the country. And using the effects identified in my paper, I simulate how many fewer infections and deaths there might have been between February and mid-May 2020 if the minimum wage in all jurisdictions was 10 percent higher. Finally, I examine several policies that states and the federal government could consider in order to improve the quality of care in eldercare residential settings over the longer term, among them:
- Raise the federal minimum wage to boost the wages of low-wage workers in eldercare facilities
- Structure Medicare reimbursement rates for eldercare facilities to further incentivize high-quality care
- Incorporate staffing costs into Medicaid reimbursement rates so that eldercare facilities that pay workers higher wages receive slightly higher revenue
Importantly, many of these reforms could be implemented without a substantial overhaul of existing eldercare programs or policies.
Quality and staffing in long-term care
Nursing homes provide long-term residential care on a 24/7 basis to patients who require assistance with activities of daily living, such as eating, walking, and showering. Nursing homes, like other long-term care settings, rely heavily on low-wage labor. About 40 percent of nursing home employees are nursing assistants—direct-care staff who provide the majority of person-to-person care by helping residents with activities of daily living and who work with certified nurses and eldercare teams to monitor patients’ conditions. Yet these employees, like many other essential workers in maintenance and food prep occupations, are among the lowest-paid workers in the U.S. economy. Most earn less than $14 an hour.
While existing research shows that higher staffing levels are associated with better patient outcomes, nursing homes frequently report difficulty in recruiting and retaining staff. Between 60 percent and 85 percent of nursing assistants leave their employers each year, most often to go work in other nursing homes. This turnover rate is two to three times higher than that across the entire healthcare sector.
The difficulty in staffing nursing homes 24 hours a day, 7 days a week means that in the typical eldercare facility, residents receive about 4 hours of nursing care a day: 2.3 hours from a nursing assistant and 1.6 hours from either a licenced vocational nurse or a registered nurse. These levels are below the levels many medical experts recommend, and often even lower on weekends. Moreover, staffing shortages are acute amid the current coronavirus pandemic as workers and their families become exposed to the virus and contract COVID-19.
Taking a step back, there are several channels by which higher wages could improve patient care and firm performance. First, standard “efficiency wage” models in economics posit that paying workers higher wages incentivizes better performance by making unemployment and the loss of a paycheck more “costly” to workers. Second, an emerging literature in psychology and economics documents that financial pressures and the stress associated with poverty impair cognitive functioning—stress that could be allieviated by paying low-wage workers higher wages to improve household budgets and improve overall financial decisionmaking. Third, when a firm offers higher wages, competing firms are less likely to poach workers by offering even higher pay. This means the hiring and training costs associated with turnover fall, and the workers who stay with their employers for longer periods gain firm-specific expertise and become even more productive.
These mechanisms to improve eldercare in nursing homes by improving workers’ pay may seem intuitive. But there is relatively little empirical work on whether higher wages can improve the quality of goods and services customers receive, particularly in the low-skilled service industries where worker performance is not systematically monitored and measures of quality are often subjective. In order to make progress on this question, in my working paper, I combine information on statutory minimum wages at the federal, state, and city levels with administrative data on nursing home inspection violations, resident health, and mortality.
My findings indicate that even before the recent pandemic, many eldercare-facility residents faced day-to-day conditions that put their health and safety at risk. In the most recent inspection data, more than a quarter of facilities received a violation related to infection control and prevention. Moreover, between 2008 and 2012, 20 percent of residents who entered a nursing home after a hospital discharge were readmitted to the hospital within a month for harm that was fully avoidable, according to the Department of Health and Human Services’ Office of the Inspector General.
Simply relating wage levels in an area to patient outcomes probably misses important factors that might influence both the minimum wage and the health of the elderly in these care facilities, such as demographic patterns, economic conditions, and other policies. In order to overcome this empirical challenge, my approach leverages the fact that businesses in the same geographic area can face different minimum wages when cities, states, and counties raise the minimum wage, depending on what side of the border these establishments operate. Using this fact, I compare changes in patient outcomes within a nursing home before and after the minimum wage increases, relative to changes in a neighboring facility that does not experience the same change in the minimum wage.
This approach largely compares facilities on both sides of a state border, such as Illinois and Indiana, but also includes county- and city-level reforms by comparing, for example, changes in facilities in Chicago relative to those in neighboring DuPage County. I then aggregate all of these “county-pair” comparisons over a 25-year period in order to estimate the effect of the minimum wage on worker, resident, and firm well-being.
I first show that when the minimum wage increases, nursing assistants and other less-skilled staff receive a pay increase. The most recent federal increase between 2007 and 2009, from $5.15 per hour to $7.25 per hour, for example, increased nursing assistants’ annual pay by between 5 percent to 8 percent (about $1,300 to $2,300) with no significant reduction in the number of nursing assistants employed or the time spent with residents. At the same time, higher wages reduced the separation rate (that fraction of workers who leave their employers) and increased the fraction of stable hires (that share of new hires who remain with their new employers for at least 3 months). These patterns mean that, on the whole, workers gain firm-specific expertise and receive additional income, but do not lose their jobs.
Second, I show these minimum wage induced increases in pay for nursing home staff improve health and safety conditions for patients. My working paper finds that increasing the minimum wage by 10 percent would reduce the number of health inspection violations by 1 percent to 2 percent, the number of residents with moderate to severe pressure ulcers by about 1.7 percent, and the number of deaths by 3 percent.
What do these patterns mean for firms? Using financial report data, I show that after a minimum wage hike, eldercare facilities report that their costs increase by the same amount as the increased labor costs, and they fully recoup these costs by charging residents higher prices. These price increases are concentrated among residents who are paying out of pocket, rather than those covered by Medicaid or Medicare, and, at the same time, these facilities admit slightly more private payors, fewer Medicaid residents, and do not change the number of Medicare recipients. Importantly, however, I do not find a significant increase in deaths occurring outside nursing homes, suggesting that consumers are able to find care options that are equivalent in quality, at least on this dimension.
COVID-19 and nursing homes
What do these patterns mean amid the current coronavirus pandemic and the rising number of COVID-19 cases and deaths in nursing homes? And to what extent are observable factors associated with a recent outbreak in specific eldercare facilities? In April 2020, the federal Centers for Medicare & Medicaid Services, or CMS, issued guidance requiring nursing homes to submit information on COVID-19 cases and deaths among residents and staff to the Centers for Disease Control and Prevention, yet these data are not yet publicly available, and other measures of patient care during the pandemic will not be available for several months.
So, as a preliminary step to provide some insights about what types of long-term care settings have documented cases of COVID-19, I match facility-level information on the number of cases and deaths collected by The New York Times through May 9, 2020 to CMS administrative reports on inspection violations, staffing levels, and patient health outcomes from the most recent inspection period (2019 through February 2020). As reporting requirements vary by state and measures are not comparable across states, all of these figures show patterns in facilities with known COVID-19 deaths relative to facilities in the same state without known deaths.
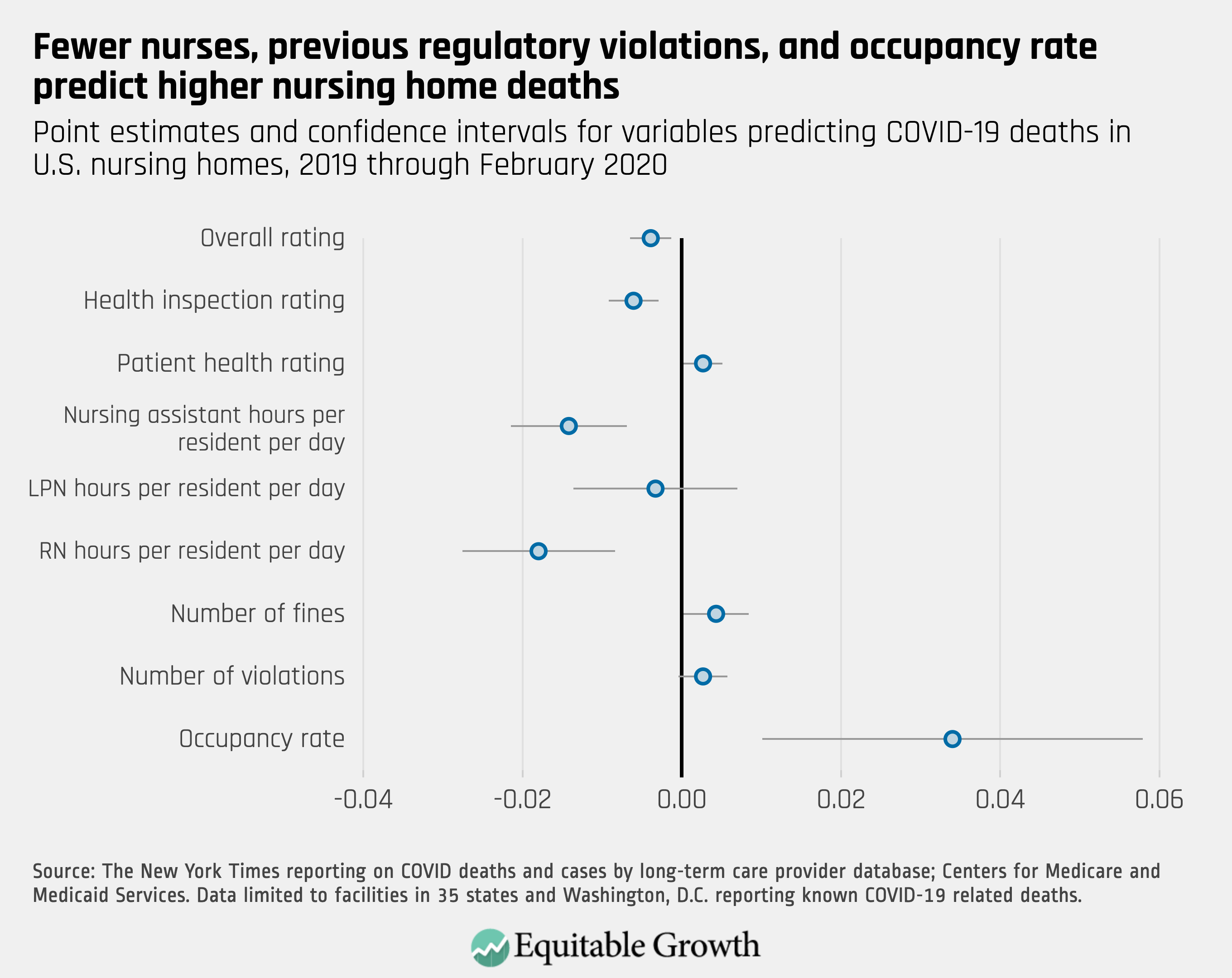
The data provide some suggestive evidence that higher service quality is associated with fewer deaths from COVID-19 in nursing homes. Facilities with documented COVID-19 deaths tend to have lower nurse staffing levels, more inspection violations and fines, and operate closer to full capacity than facilities in the same state without such violations. (See Figure 1.)
Figure 1
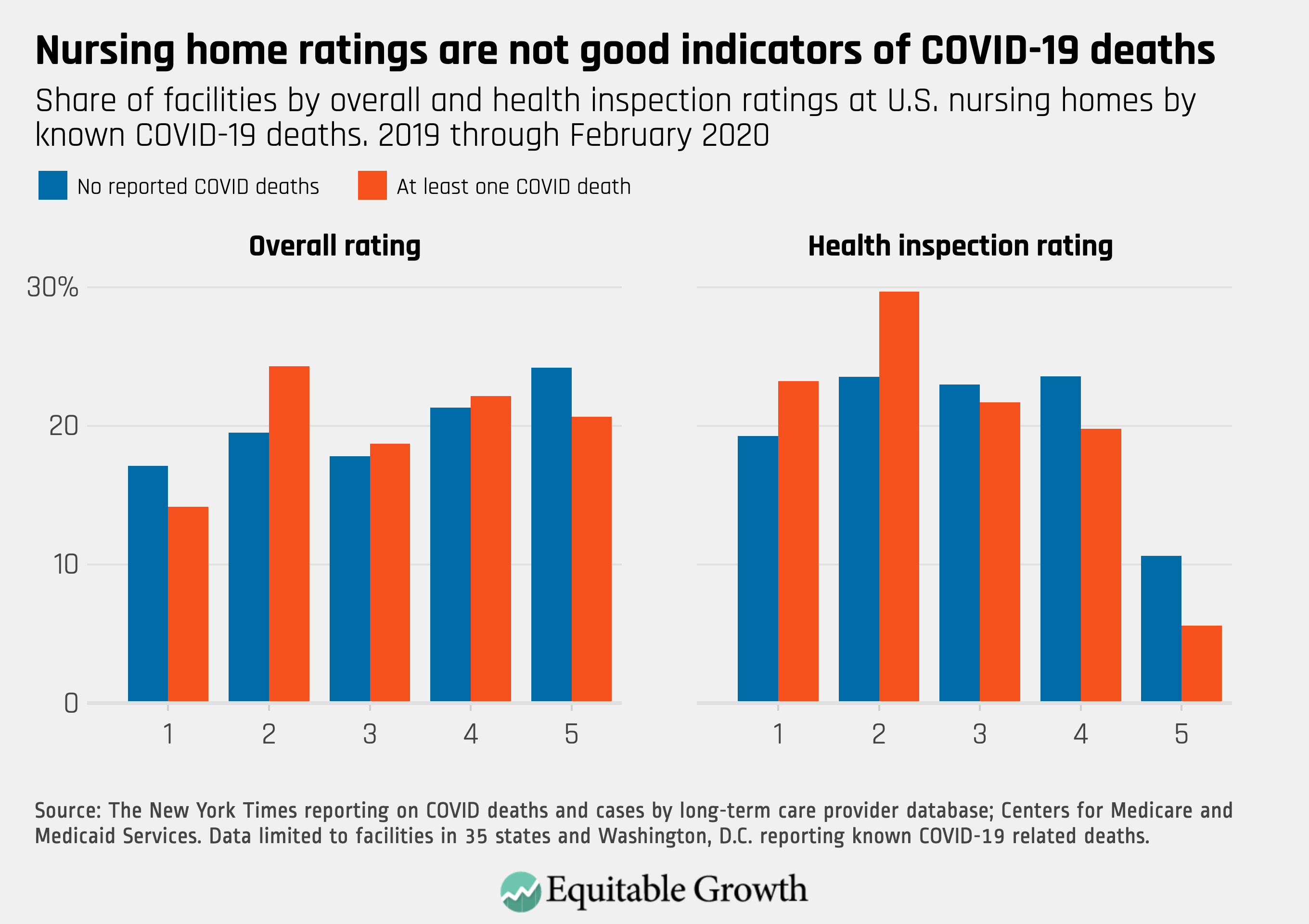
These average differences are small, and many facilities with documented outbreaks are among the highest-rated centers. The data show that, for example, more than 40 percent received a four- or five-star overall rating, and more than a quarter received at least four stars on the most recent health inspection. (See Figure 2.)
Figure 2
As a second analysis, I apply the estimates on improvements in patient health and safety to a hypothetical reform that would increase the minimum wage by 10 percent in all jurisdictions. So, for example, the federal minimum would increase to just less than $8; states with a minimum of $10 would increase their minimum to $11; and some of the highest minimum wage jurisdictions, such as San Francisco and New York City, would increase their minimum from $15 to $16.50 an hour. Between February 1 and March 16, 2020, more than 170,000 residents died in eldercare facilities, from both COVID-19 and other causes. My estimates imply that this hypothetical reform could have prevented at least 5,300 of these deaths, or about 3 percent.
I can also extend the approach in my paper to focus on infection-related violations and deaths specifically. Here, I find that with a 10 percent minimum wage increase, over the course of the year, 200 fewer eldercare facilities would receive any infection-control violations, and the total number of such violations would fall by 5 percent. Finally, the number of eldercare facility deaths due to infection would fall by 3.3 percent.
Although these estimated reductions may seem small in the context of the overall COVID-19 death toll, now surpassing 100,000 nationwide, it is important to recognize that such a reform comes at a modest cost. Increasing the minimum wage everywhere in the country by 10 percent would increase each nursing assistant’s annual pay by about $350 to $600, meaning that the cost of each eldercare facility death prevented in early 2020 ranges from $38,000 to $70,000, below existing estimates of quality-adjusted life years saved for the elderly population.
Conclusion and policy options
Even before the COVID-19 crisis amplified concerns about resident safety and health in long-term eldercare settings, our nation was already facing another potential health crisis with the baby boomer generation entering retirement and demand for long-term care increasing commensurately. Over the next several decades, the costs to Medicare and Medicaid will likewise increase, making it even more critical that we promote policies that promote both residents’ health and workers’ livelihoods. My working paper points to one such policy reform: increasing pay for healthcare support staff. Fortunately, there are several modest policy changes that federal, state, and local government officials could pursue now in order to incentivize better care.
Perhaps the most obvious reform, and directly tied to my work, is to increase workers’ pay. While many states and localities have taken recent action to increase their minimum wages, at $7.25 an hour, the federal minimum wage means that a full-time worker supporting a family of three earned about 73 percent of the federal poverty line in 2019, the lowest level since 2008. My results suggest if the federal government just increased the federal minimum wage by 10 percent, then average nursing assistant earnings would increase by about $325 to $560 a year, and at least 7,000 nursing home deaths could be prevented each year in just the 21 states subject to the federal minimum.
Increasing the federal minimum wage also would increase earnings and increase retention for other essential low-wage occupations, such as grocery clerks, food service workers, and retail employees, during this coronavirus pandemic. Beyond this broad policy reform, however, there are several targeted changes policymakers could enact for the long-term eldercare sector.
First, most long-term eldercare stays are covered by Medicaid and Medicare. In the case of Medicare, the recent Skilled Nursing Facilities Value-Based Purchasing Program has provided small financial incentives for facilities to lower their hospital readmission rates by increasing reimbursements for facilities with lower-than-expected rates and by decreasing reimbursements for those readmitting more residents than expected. Recent research by Tamara Konetzka at the University of Chicago, Meghan Skira at the University of Georgia, and Rachel Werner at the University of Pennsylvania shows performance-based payment formulas, particularly those with simple structures, can improve targeted outcomes. While the coming years will provide more information on whether the size of this program is an adequate incentive, policymakers may wish to further structure reimbursement rates to incentivize high-quality care.
For residents covered by Medicaid, the most common payment source, states have substantial flexibility in structuring reimbursement formulae and rates. Some states, such as California and Washington, explicitly incorporate staffing costs into their formulas so that facilities that pay workers higher wages receive slightly higher revenue. The effects of these policies have not yet been fully explored in the public health literature, but my findings suggest that if firms are able to cover higher labor costs without losing profits, then they avoid reducing staffing levels, and patient health and safety correspondingly improves.
—Krista Ruffini is a visiting scholar at the Minneapolis Federal Reserve. She is a 2019 Equitable Growth grantee.